Coronary Calcium Score: What CT Scans Reveal About Plaque
Why Silence Kills Hearts
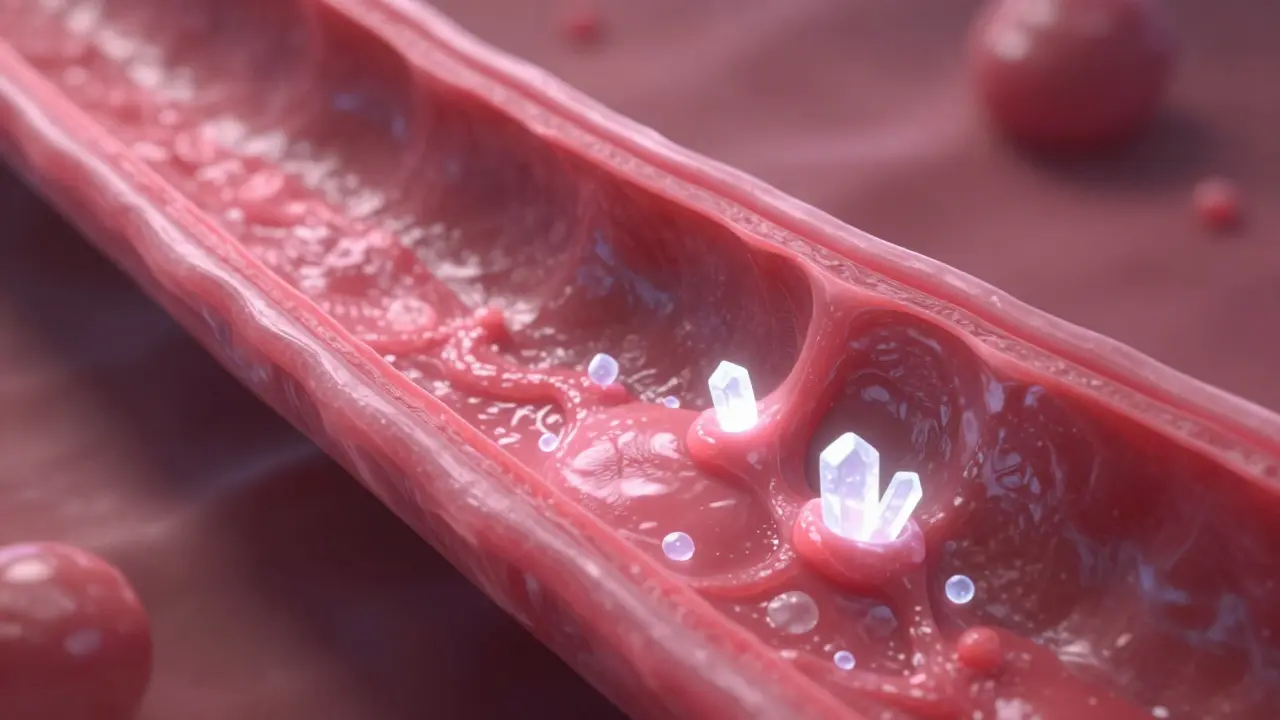
You might feel fine today, eat decent food, and even exercise occasionally. Yet, your arteries could be silently clogging up. This is the brutal reality of Coronary Artery Disease is a condition where plaque builds up in the coronary arteries, restricting blood flow to the heart muscle. The problem is that soft plaque is invisible to standard X-rays and often causes no symptoms until a heart attack happens. However, when that hardens into calcium, we can see it. That visibility is the power of the Coronary Calcium Score is a quantitative measurement of calcified plaque in the heart arteries using computed tomography technology. It turns a silent threat into a number you can actually fight.
The Mechanics of Seeing the Invisible
Most people associate heart scans with contrast dye running through their veins or strenuous treadmill sessions. Neither applies here. This procedure uses a specialized version of Computed Tomography is an imaging technique that uses X-ray technology to create cross-sectional images of internal body structures, commonly known as a CT scanner. It captures images of your chest without injecting any dye. Because calcium blocks X-rays differently than soft tissue, the machine highlights areas of plaque buildup instantly.
The process is remarkably quick. You lie flat on the scanning table, and sensors attach to your chest to monitor your heart rhythm. You hold your breath for about ten seconds. That is all it takes. The Multidetector CT is a modern imaging device capable of acquiring multiple image slices simultaneously, allowing for high-speed cardiac imaging then processes these images into a three-dimensional map of your heart. The beauty lies in the safety profile too. The radiation dose is low, typically ranging from 1 to 3 millisieverts, which is roughly comparable to a few months of natural background radiation exposure or similar to a mammogram.
Decoding the Numbers: The Agatston Scale
Once the images are processed, radiologists look for white spots within the vessel walls. These aren't random noise; they represent years of arterial damage. To turn those spots into actionable data, doctors use the Agatston Score is the standard calculation method for quantifying the amount of coronary artery calcium based on area and density. Arthur Agatston developed this system back in 1990, and it remains the industry standard today.
The calculation multiplies the size of each calcified lesion by a density factor. The result is your total score. But what does that number mean for you? Here is how the ranges break down:
| Score Range | Plaque Burden | Clinical Implication |
|---|---|---|
| 0 | No detectable calcium | Very low short-term risk of heart event |
| 1-10 | Minimal plaque | Lifestyle changes recommended |
| 11-100 | Mild plaque | Moderate risk; consider statins depending on other factors |
| 101-400 | Moderate plaque | Elevated risk; aggressive risk factor management needed |
| 401+ | Extensive plaque | High risk; warrants intensive treatment and monitoring |
A score of zero is the gold standard. It suggests you do not have significant calcified plaque, offering a strong reassurance of low immediate risk. However, anything above zero indicates that Atherosclerosis is a systemic disease characterized by the buildup of fatty deposits and calcified plaque in the arterial walls is present somewhere in your heart's arteries. The higher the number, the more material there is. For context, a person in their 40s with a score over 100 is significantly ahead of the curve, while a 70-year-old might naturally carry some calcium.

Is This Better Than Standard Tests?
Doctors have used risk calculators for decades. You fill out a form with your age, blood pressure, and cholesterol levels. These tools estimate your ten-year risk of a cardiovascular event. While helpful, they rely on population averages. They cannot see your personal biology. Research published in major journals shows that traditional calculators misclassify about 20 to 30 percent of patients in the intermediate risk group. Some get flagged as high risk when they are fine, while others are marked safe when they are not.
This is where the calcium scan adds precision. It reclassifies risk for nearly half of these borderline cases. Consider the scenario where a patient has normal cholesterol but carries heavy calcification. The standard calculator says wait and watch. The scan says treat now. Conversely, if you have high cholesterol anxiety but a scan score of zero, your doctor might de-intensify medication plans safely.
It also holds an edge over Stress Testing is a diagnostic procedure that evaluates heart function during physical exertion to identify blockages. Stress tests check for reduced blood flow caused by blockages. Calcium scoring checks for the presence of the blockage itself before it causes ischemia. There is a caveat, though. This scan only sees hard, calcified plaque. Non-calcified, soft plaque remains invisible. This accounts for roughly 20 to 30 percent of plaque volume in some patients, making this tool slightly less comprehensive than a full coronary angiography, though far safer for screening purposes.
When Should You Get Tested?
Not everyone needs this scan. Guidelines from the American College of Cardiology is a professional association representing physicians dedicated to the practice of cardiology recommend it primarily for asymptomatic adults aged 40 to 75 who fall into that intermediate risk category. If your calculated risk is already very low, the scan adds little value. If your risk is extremely high due to a history of heart attacks or diabetes, you probably already know you need aggressive care regardless of the score.
However, family history changes things. If your father had a heart attack at 45, you are carrying a genetic load that standard math might miss. Recent guidelines expanded eligibility to include anyone with LDL cholesterol above 160 mg/dL in their 40s, even without other risk factors. This shift acknowledges that biological risk often appears early. For women, particularly post-menopausal, this test is becoming increasingly valuable as traditional risk factors lose their predictive power compared to actual arterial evidence.

Treatment Implications: Moving from Fear to Action
Finding a high score can feel terrifying. Seeing "250" on a report feels like a death sentence, but it is actually a wake-up call. The data shows that acting on these numbers saves lives. A score between 100 and 300 generally triggers a recommendation for moderate-intensity Statin Therapy is a class of drugs that lower cholesterol by inhibiting enzyme production in the liver. If your score exceeds 300, clinicians typically recommend high-intensity regimens. Why? Because stabilizing plaque prevents rupture. Even if you cannot remove the calcium, stopping the growth of new plaque reduces the likelihood of a clot forming and cutting off blood flow.
Patient anecdotes highlight this psychological impact. One individual shared that seeing a score of 142 motivated him to finally quit smoking after years of ignoring warnings. The visual proof of damage was more persuasive than verbal advice. The scan provides leverage for behavior change. It transforms abstract concepts like "cholesterol" into concrete physical evidence of wear and tear on your heart.
Navigating Costs and Coverage
One of the biggest hurdles is money. In many regions, public health systems do not cover this test routinely. Private insurance might require specific risk criteria to approve the claim. Without prior authorization, out-of-pocket costs often range between $100 and $300. In places like North America, Medicare generally excludes this for average wellness visits, reserving it for specific diagnostic needs. This creates a barrier for prevention. If you are uninsured or have high-deductible plans, ask your facility for a cash-pay price list before booking.
Furthermore, access depends on the facility having the right equipment. Older machines struggle with motion artifacts from beating hearts. Modern 64-slice or higher scanners handle the rapid imaging required accurately. Ensure the center performing your scan specializes in cardiac imaging. Generic radiology centers might miss subtle calcium deposits or trigger false positives due to motion blur.
Living With the Results
If your score is elevated, you do not panic. You plan. Repeat testing every 10 to 20 years allows you to track progression. If you are doing the lifestyle work-diet, exercise, smoking cessation-and your score remains stable upon retesting, that confirms success. Rapid increases signal a need for stricter intervention. Regular follow-ups keep the focus on long-term preservation rather than immediate crisis management.
Does a zero score mean I am immune to heart disease?
A score of zero indicates no detectable calcified plaque. This significantly lowers your short-term risk of a heart event. However, it does not rule out the presence of soft, non-calcified plaque entirely, so maintaining a healthy lifestyle is still essential.
How often should I repeat the scan?
For most people, repeating the scan every five years is sufficient if the initial score was above zero. If your score is 100 or higher, your doctor may suggest shorter intervals to monitor the effectiveness of medication and lifestyle changes.
Is there radiation risk involved?
The procedure involves low-dose radiation, approximately 1 to 3 mSv. This is comparable to natural background radiation received over several months and is considered safe for screening purposes by major health organizations.
Can I prepare specifically for the test?
You generally need to avoid caffeine and nicotine for four hours prior to the exam. These substances elevate your heart rate, which can blur the images. Wear comfortable clothing without metal zippers or jewelry.
Will my doctor change medications based on the score?
Yes. Scores above 100 often warrant starting or increasing statin therapy. Scores near zero might allow for medication reduction if your doctor determines your overall risk profile supports it.


walker texaxsranger
March 28, 2026 AT 21:10The radiology industry pushes calcification metrics because it drives revenue streams for CT maintenance contracts rather than genuine patient outcomes studies showing actual mortality benefit reduction in asymptomatic cohorts soft plaque rupture remains the primary mechanism for acute myocardial infarction events yet this scan misses those completely invisible high-risk lesions entirely we are prioritizing density over flow dynamics which creates false reassurance scenarios where patients delay necessary angiographic intervention due to negligible scores insurance mandates require documented risk factors before authorization but private payers often bypass these protocols creating inequality in diagnostic access across socioeconomic strata radiation exposure adds stochastic cancer risks even at millisievert levels which contradict the prevention narrative sold to anxious demographic groups seeking validation biomarkers like lipoprotein subfraction analysis provide superior predictive value without the ionizing burden inherent in tomography hardware systems designed decades ago
kendra 0712
March 29, 2026 AT 16:58But but but!!! You are missing the main point!!!!! It really helps people wake up!!! My friend got his done last week!!! He was shocked by the numbers!!!!! It changed everything for him!!!!!!
Debra Brigman
March 30, 2026 AT 07:31The heart whispers secrets through calcium deposits like an old diary hidden beneath layers of mundane tissue waiting for the brave to uncover its truths we chase shadows on screens hoping to catch a glimpse of our own mortality quantified in cold integers rather than accepting the fluid chaos of human biology modern medicine demands certainty while life insists on ambiguity and we sit in the grey zone demanding answers from machines built of glass and wire sometimes seeing the ghost is worse than fearing it lurks unseen in the dark corridors of our veins we seek control over the inevitable decay that awaits us all regardless of what the scanner reveals in its digital gaze
Rachael Hammond
March 31, 2026 AT 02:03i think u guys are both rite kind of like sometimes too much tech feels weird but knowing the truth is good too my mom had her done last yr and she cried when they showed the pics on the screen she started walking everyday after that and stopped eating sugar totally im trying to figure out if i should get one this winter maybe doctors usually dont talk about it unless you push them i guess hope everyone stays healthy out there for real
Tony Yorke
April 1, 2026 AT 07:52good info definitely going to check mine soon
Devon Riley
April 1, 2026 AT 15:34Everyone deserves peace of mind regarding their own health journey 🧠❤️ Seeing the data clearly removes the fog of anxiety that clouds decision making 🌟 It is amazing how tangible evidence shifts perspective towards better choices immediately 💪🏃♂️ We should encourage friends to take charge instead of waiting for symptoms to appear 🚨 Prevention starts with awareness and knowledge is truly power in this scenario 🔓 Keep looking after yourselves out there please 🙏🏽
Kameron Hacker
April 3, 2026 AT 00:23While sentimentality is acceptable in social contexts rigorous adherence to evidence-based guidelines supersedes emotional appeals regarding diagnostic utility your assertion ignores the statistical significance required to validate screening interventions in low risk populations devoid of clinical indications emotional support does not mitigate biological degradation occurring independent of perceived safety measures derived from superficial scanning procedures we must prioritize efficacy over empathy in public health policy formulation involving radiation exposure justification frameworks sentimental reasoning fails to address the systemic allocation of resources which impacts broader community health outcomes negatively
Poppy Jackson
April 3, 2026 AT 00:52imagine finding out your heart has been fighting a silent war inside you all along without you knowing anything about it it makes you tremble just thinking about the damage quietly building up year after year tears welling up whenever the doctor mentions a score above zero honestly we need to act fast before the darkness takes over our future completely this scares me deeply but also empowers me somehow weirdly
Rohan Kumar
April 3, 2026 AT 01:08sure keep panicking about invisible ghosts while the real issue is sitting right in front of you 🙄 the system is just trying to scare you into paying for unnecessary scans 🤑 stop crying over numbers nobody understands anyway 🙃🔥
Paul Vanderheiden
April 3, 2026 AT 17:06it takes courage to look at the truth but you must embrace it fully the numbers do not define who you are but they show where you stand today ignoring the warning signs only leads to bigger problems later down the road for sure many people think they feel fine until the pain hits unexpectedly and then it is too late you have the power to change the outcome starting with what you eat daily small steps towards better habits create massive improvements over time consistently do not let fear paralyze you from taking action right now today every day you live clean is a victory against the aging process naturally talk to your team and trust that they want you safe and sound always remember why you started this journey to protect your loved ones nearby staying informed keeps you ahead of potential threats lurking in the background celebrate the wins no matter how minor they might seem at first glance you are stronger than the obstacles standing directly in your path right now stay focused on the goal of a healthy heart beating strong forever believe in your ability to overcome whatever challenges arise during treatment phases most importantly love yourself enough to make the changes needed for longevity
Tommy Nguyen
April 4, 2026 AT 13:12totally agree with that mindset positive vibes help everything heal faster