Sitagliptin‑Metformin Combination: Benefits, Risks & What to Expect

When doctors prescribe Sitagliptin‑Metformin therapy is a fixed‑dose combination of the DPP‑4 inhibitor sitagliptin and the biguanide metformin, used primarily for type 2 diabetes, they’re aiming for a single pill that tackles blood‑sugar spikes, weight gain, and heart‑health concerns all at once. The idea sounds simple, but the real‑world picture is a mix of solid data, patient experiences, and a few gray zones.
Why put sitagliptin and metformin together?
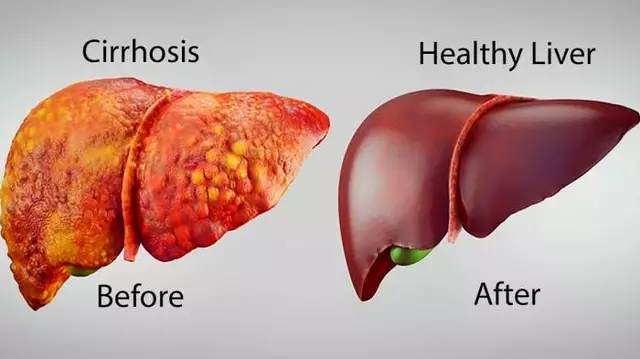
Metformin has been the first‑line therapy for decades. It lowers glucose production in the liver and improves insulin sensitivity, which usually translates into a 1‑1.5% drop in HbA1c. Sitagliptin belongs to the DPP‑4 inhibitor class; it boosts the body’s own incretin hormones, leading to more insulin release after meals without a big risk of hypoglycemia.
When you stack them, you hit two major pathways: fasting glucose (metformin) and post‑prandial spikes (sitagliptin). The synergy often means you can stay under the target HbA1c with a lower dose of each drug, potentially reducing side‑effects tied to higher doses.
Key advantages of the combo
- Improved glycemic control: Clinical trials show an average HbA1c reduction of 0.8-1.2% compared with metformin alone.
- Weight neutrality: Sitagliptin doesn’t add weight, and metformin can even promote modest loss. Patients rarely report the weight gain seen with sulfonylureas.
- Low hypoglycemia risk: Because neither drug forces insulin release, the combo is safe for most patients, even the elderly.
- Convenient dosing: One pill a day simplifies regimens, boosting adherence.
- Cardiovascular safety: The Cardiovascular Outcomes Study of Sitagliptin (CAROLINA) found no increase in major adverse cardiac events compared with standard therapy.
Potential drawbacks to watch
- Gastro‑intestinal upset: Metformin’s classic nausea, diarrhea, and bloating can still surface, especially during the first weeks.
- Pancreatitis concern: DPP‑4 inhibitors carry a rare (<0.1%) risk of pancreatitis; physicians usually screen for a history of pancreatic disease.
- Renal dosing limits: Both drugs are cleared by the kidneys. In patients with eGFR < 30 mL/min/1.73 m², dose reductions or alternatives are recommended.
- Cost: The brand‑name fixed‑dose combo can be pricier than separate generic tablets, though many insurance plans now cover it.
- Limited dose flexibility: If a patient needs a higher dose of metformin but not sitagliptin, the combo forces unnecessary exposure to sitagliptin.

What the research says
Several randomized controlled trials (RCTs) and real‑world cohort studies have examined the combo. A 2023 meta‑analysis of nine RCTs involving 4,860 participants reported a mean HbA1c reduction of 0.95% versus metformin monotherapy, with a relative risk of gastrointestinal adverse events of 1.27 (still acceptable for most). The sitagliptin metformin fixed‑dose also showed a 15% higher medication‑adherence rate compared with taking two separate pills.
When you compare the combo to newer agents like GLP‑1 receptor agonists, the picture changes. GLP‑1 drugs often deliver greater weight loss (3‑5 kg) and a stronger cardiovascular benefit, but they require injections and have higher rates of nausea. For patients who prioritize oral therapy and cost, sitagliptin‑metformin remains a solid middle ground.
Who should consider the combo?
Guidelines from the American Diabetes Association (ADA) and the Canadian Diabetes Association (CDA) list the combination as a reasonable second‑line option after metformin failure, especially when:
- The patient is overweight or obese but not ready for injectable therapy.
- Renal function is stable (eGFR ≥ 45 mL/min/1.73 m²) and no history of pancreatitis.
- Cost is a concern and the patient benefits from a single‑pill regimen.
Conversely, avoid it in patients with severe renal impairment, those prone to recurrent GI upset, or those already on high‑dose metformin where the fixed dose would limit titration.
Practical prescribing tips
- Start low: Many clinicians begin with the 50 mg sitagliptin / 500 mg metformin tablet, then titrate up to the 100 mg / 1000 mg strength after two weeks.
- Split the dose if needed: For patients with GI sensitivity, taking the tablet with dinner instead of breakfast can soften the stomach upset.
- Monitor labs: Check HbA1c every 3 months, and repeat eGFR and liver function tests at baseline and annually.
- Educate on symptoms: Advise patients to report persistent abdominal pain, vomiting, or sudden weight loss, which could hint at pancreatitis.
- Insurance check: Verify coverage before the first fill; many provincial plans in Canada list the combo under Tier 2, requiring a modest co‑pay.

How does it stack up against alternatives?
| Regimen | HbA1c reduction | Weight impact | Hypoglycemia risk | Typical cost (CAD/month) |
|---|---|---|---|---|
| Metformin alone | ~0.8‑1.0% | ‑0.5 kg | Low | $5‑10 (generic) |
| Sitagliptin‑Metformin combo | ~0.9‑1.2% | Neutral | Low | $40‑60 (brand) |
| Sulfonylurea + Metformin | ~1.0‑1.4% | +1‑2 kg | Moderate‑High | $15‑25 (generic) |
| GLP‑1 agonist (oral) + Metformin | ~1.2‑1.6% | ‑3‑5 kg | Low | $120‑150 |
Notice the combo sits in a sweet spot: better HbA1c than metformin alone, but without the weight gain and hypoglycemia of sulfonylureas, and far cheaper than GLP‑1 agents.
Bottom line for patients and clinicians
If you’re a person with type 2 diabetes who has already tried metformin and needs a modest extra push, the sitagliptin‑metformin pill often delivers that boost with minimal hassle. It’s especially attractive for folks who dislike injections, have modest kidney function, and want to keep their out‑of‑pocket costs reasonable.
However, it’s not a magic bullet. Those with a history of pancreatitis, severe renal disease, or who experience persistent GI distress may fare better with an alternative class. As always, the decision should be a shared one-talk to your healthcare provider about your lifestyle, lab results, and any concerns you have.
Frequently Asked Questions
Can I take sitagliptin‑metformin if I’m already on separate metformin and sitagliptin tablets?
Yes. Switching to the fixed‑dose combo simplifies your regimen, but make sure the total daily dose of each component matches what you were already taking. Your doctor may adjust the strength to avoid over‑ or under‑dosing.
What should I do if I experience stomach upset after starting the combo?
Take the pill with a full glass of water and a meal. If diarrhea persists beyond two weeks, contact your prescriber-sometimes a slower titration or a temporary switch to separate tablets helps.
Is the combination safe during pregnancy?
Metformin is generally considered safe in pregnancy, but sitagliptin is classified as Category C. Most clinicians prefer to discontinue sitagliptin and manage blood sugar with insulin or metformin alone.
How often should I have my kidney function checked?
At least once a year if your eGFR is above 60 mL/min/1.73 m². If you’re borderline (45‑60), check every six months. Adjust the dose or switch therapy if the eGFR falls below 45.
Does insurance usually cover the combo?
In Canada, most provincial drug plans list the combination under the generic tier for patients with a diabetes benefit. Private insurers often cover it, though a modest co‑pay is typical. Always verify with your pharmacy before filling.


Samantha Vondrum
October 24, 2025 AT 12:15The combination of sitagliptin and metformin represents a thoughtful evolution in type 2 diabetes management, aiming to address both fasting and post‑prandial glucose excursions in a single tablet. Clinical data indicate that the duo can lower HbA1c by roughly 0.8 to 1.2 percentage points, which is comparable to many dual‑therapy regimens. Moreover, the weight‑neutral profile of sitagliptin paired with the modest weight‑loss effect of metformin provides an advantage over sulfonylureas that often promote gain. Patients also benefit from a reduced pill burden, which has been shown to improve adherence, especially among older adults. The cardiovascular safety signals from the CAROLINA trial reassure clinicians that sitagliptin does not increase major adverse cardiac events. Gastro‑intestinal side‑effects, such as nausea and diarrhoea, remain largely attributable to the metformin component and typically subside after dose titration. It is essential to counsel patients to take the medication with meals to mitigate these effects. Renal function should be assessed before initiation, as metformin accumulation can occur in severe impairment. Lifestyle modifications, including diet and exercise, remain the cornerstone and should accompany pharmacotherapy. The cost of the fixed‑dose combination can be higher than separate generic agents, which may affect accessibility for some individuals. Nonetheless, many insurance plans now cover the combo, recognizing its adherence benefits. Physicians should individualize dosing, sometimes starting with a low dose of each agent to improve tolerability. Monitoring should include periodic HbA1c checks, renal function tests, and assessment of gastrointestinal symptoms. In the event of persistent intolerance, reverting to separate agents or adjusting the metformin dose may be warranted. Overall, the sitagliptin‑metformin fixed‑dose offers a balanced approach that aligns efficacy, safety, and convenience. 😊📊
Future research may clarify its role in specific subpopulations, such as those with heart failure or chronic kidney disease.
Shirley Slaughter
October 25, 2025 AT 06:20When you think about the daily battle against sugar spikes, the sitagliptin‑metformin duo feels like a heroic alliance, marching onto the stage of diabetes care with trumpets blaring. The synergy between fasting glucose control and post‑meal insulin release creates a crescendo of stability that many patients long for. Imagine a world where a single pill can tame the wildest cravings while keeping the weight scale from tipping over – pure drama turned into reality. Yet, the plot thickens with gastrointestinal side‑effects that can linger like an unwanted encore. Clinicians must play the role of wise directors, guiding dosage titration with patience and compassion. In the grand narrative of therapy, this combination writes a chapter of hope and caution alike. 🎭
Narasimha Murthy
October 26, 2025 AT 02:13While the trials sound impressive, the real‑world adherence data are far less rosy, and many patients still discontinue due to GI upset. The claim of “weight neutrality” is overstated; metformin‑induced loss is modest at best. Moreover, the cost premium of the fixed‑dose often outweighs the marginal HbA1c advantage.
Suraj 1120
October 26, 2025 AT 20:23The pharma machines designed this combo to lock you into a lifelong subscription, not to solve any medical mystery. They hide the fact that sitagliptin’s rare pancreatitis risk is brushed under the carpet while pushing a glossy marketing narrative. If you value independence, demand a breakdown of each component rather than swallowing a packaged pill.
Joey Yap
October 27, 2025 AT 14:33In the mosaic of chronic disease management, each medication is a tile that must fit both the clinical picture and the patient’s lived experience. The sitagliptin‑metformin pair offers a harmonious blend of mechanisms, yet harmony is incomplete without the patient’s voice. Encouraging shared decision‑making can transform a prescription from a static directive into a collaborative journey. When patients understand why each pill matters, adherence becomes a natural expression of self‑care. Ultimately, the therapy’s success is measured not just in numbers but in the quality of daily life.
Lisa Franceschi
October 28, 2025 AT 08:43From a pharmacological standpoint, the fixed‑dose formulation simplifies titration schedules and reduces the likelihood of dosing errors. It is advisable to assess renal function prior to initiation, given metformin’s contraindications in severe impairment. Patients should be counselled on taking the medication with meals to minimize gastrointestinal discomfort. Regular monitoring of HbA1c and renal parameters remains essential to ensure ongoing safety and efficacy.
Diane Larson
October 29, 2025 AT 02:53One practical tip for newcomers is to start with the lowest available dose and gradually increase over two to three weeks; this often eases the stomach upset that metformin can cause. Pairing the medication with a high‑fiber breakfast can further blunt any residual nausea. If weight loss is a goal, combining the combo with a modest exercise routine amplifies the modest benefit already seen with metformin. Keep an eye on any unexplained abdominal pain, as it could signal the rare pancreatitis risk linked to DPP‑4 inhibitors. Overall, the regimen works best when it’s part of a broader lifestyle plan rather than a standalone solution.
Michael Kusold
October 29, 2025 AT 21:03i tried the combo a few months back, kinda felt the tummy stuff at first but it settled after a week. the sugar numbers dropped decent, tho not magic. definitely easier than popping two pills.
Selina M
October 30, 2025 AT 15:13Love how simple the once‑daily dosing is! 😃
tatiana anadrade paguay
October 31, 2025 AT 09:23It’s great to see patients getting a treatment that bridges efficacy and convenience, but remember that education is key to success. Explain how sitagliptin works on the incretin system while metformin tackles hepatic glucose output, so patients appreciate the “why” behind each pill. Encourage them to monitor blood glucose trends, especially after meals, to see the post‑prandial benefits. If gastrointestinal symptoms appear, suggest taking the dose with food and possibly splitting the intake if the tablet allows. Reinforce that lifestyle changes remain the foundation, and the medication is an aid, not a cure. By fostering open dialogue, clinicians can empower patients to stay engaged and confident in their regimen.
Nicholai Battistino
November 1, 2025 AT 03:33Assess renal function before starting. Adjust dose if eGFR falls below 45 ml/min.
Sean Thomas
November 1, 2025 AT 21:43The push for this fixed‑dose is nothing more than a corporate ploy to lock unsuspecting citizens into a profit‑driven monopoly, all under the guise of “convenience.” Pharma giants have quietly suppressed cheaper generic alternatives, ensuring that our healthcare system feeds their bottom line while we swallow the pills.
Aimee White
November 2, 2025 AT 15:53Behind the soothing promotional videos lies a labyrinth of shadowy experiments where secret labs test the limits of human metabolism, hoping to turn us into compliant data points for their grand designs. The “cardiovascular safety” claim is a carefully crafted illusion, a smokescreen that masks the silent, creeping risks whispered about in hushed boardrooms.
Javier Muniz
November 3, 2025 AT 10:03Hey folks, just wanted to chime in – the combo can be a real game‑changer if you’re consistent with it. I’ve seen friends drop a few pounds and keep their A1c in the target range without nasty lows. Just remember to stay hydrated and keep an eye on any gut issues early on. It’s all about pairing the meds with solid habits.
Sarah Fleming
November 4, 2025 AT 04:13Only the enlightened few discern that the “one‑pill wonder” is a veneer masking a deeper pharmacological manipulation designed to subtly rewire our endocrine autonomy. Accepting it without question aligns you with the masses succumbing to orchestrated biomedical control. Elevate your discourse, demand transparency, and reject the complacent narrative fed to the public.